Episode 156: Immune Thrombocytopenic Purpura Series, Pt 2- Relapsed/Refractory
This week, we move to the relapsed/refractory ITP setting, focusing on what options are available to patients after their initial treatment with steroids ± IVIg, which we discussed in Episode 155! If you have not done so already, definitely listen to that episode as we build on the topics discussed here today!
What are options for patients who relapse after initial therapy (see episode 155 for first line management)?
Managing a minor drop vs. a precipitous relapse:
A repeat corticosteroid course can be considered, specifically using prednisone 1 mg/kg PO.
Weekly labs should be checked to guide management. If the drop isn’t severe or precipitous, a gradual taper every 3–5 days can be implemented.
The 6-week rule: Per ASH guidelines, ensure total steroid exposure (including the taper) does not exceed 6 weeks to minimize long-term toxicities.
Prophylaxis: Remember to consider GI protection and PJP prophylaxis if longer-term steroid courses are required.
Transitioning to second-line therapies:
A rapid relapse typically flags the need to initiate second-line discussions. We lack robust predictive models to tell us who will experience a durable response versus a quick flare, making clinical intuition and patient conversation vital here.
The role of Splenectomy in 2026:
Historically, removing the spleen was the standard first-line strategy for ITP, boasting long-term remission rates of 60–70%.
Because we cannot predict who will achieve durable remission—and the procedure is irreversible—its modern role has shifted significantly. It is now reserved for patients who fail to tolerate or remain completely refractory to medical treatments for at least 1 year.
Short-term risks: Surgical complications, acute infection, and a 2- to 4-fold increase in VTE risk compared to patients who retain their spleen.
Long-term risks: Lifelong risk of severe infection from encapsulated organisms and chronic vascular complications.
Medical second-line options:
Modern management leans heavily on Thrombopoietin Receptor Agonists (TPO-RAs) and Rituximab. Choosing between them depends heavily on patient lifestyle preference, compliance, and clinical urgency, as there are no head-to-head randomized trials.
Response timelines: TPO-RAs typically work quickly (1–2 weeks), whereas Rituximab requires a longer runway (1–8 weeks).
Logistics: TPO-RAs are managed at home (pills or subQ injections), while Rituximab requires weekly outpatient infusions for a month.
Target threshold: In the second-line setting, our target platelet goal for most standard patients without severe bleeding risk factors is >50,000.
What are the options for TPO-RAs, and how do we select one over another?
Class efficacy: There are no head-to-head trials comparing individual TPO-RAs, but they are considered clinically equivalent. They feature an overall response rate of ~75% and a durable response rate (maintaining platelets >50,000) around 65%.
The available agents:
Romiplostim (N-plate): Administered as a weekly subcutaneous injection.
Eltrombopag (Promacta): A daily oral tablet. It carries strict dietary restrictions (must be taken on an empty stomach away from calcium-rich foods) and requires routine LFT monitoring due to hepatotoxicity risks.
Avatrombopag (Doptelet): A daily oral tablet. It provides a convenient alternative without the food interactions or LFT tracking requirements seen with eltrombopag.
Key clinical considerations for TPO-RAs:
Thrombosis risk: Long-term extension studies have noted an increased risk of both venous and arterial thrombotic events.
Marrow fibrosis: Early historical concerns regarding progressive bone marrow fibrosis have largely not been substantiated in practice.
Cycling therapies: If a patient fails to respond to one specific TPO-RA, switching to a different agent in the same class yields a successful response in 50–80% of cases.
Duration of treatment: This is generally considered indefinite therapy because the effects are short-lived. However, literature suggests 10–30% of patients may eventually taper and discontinue the drug while maintaining a response.
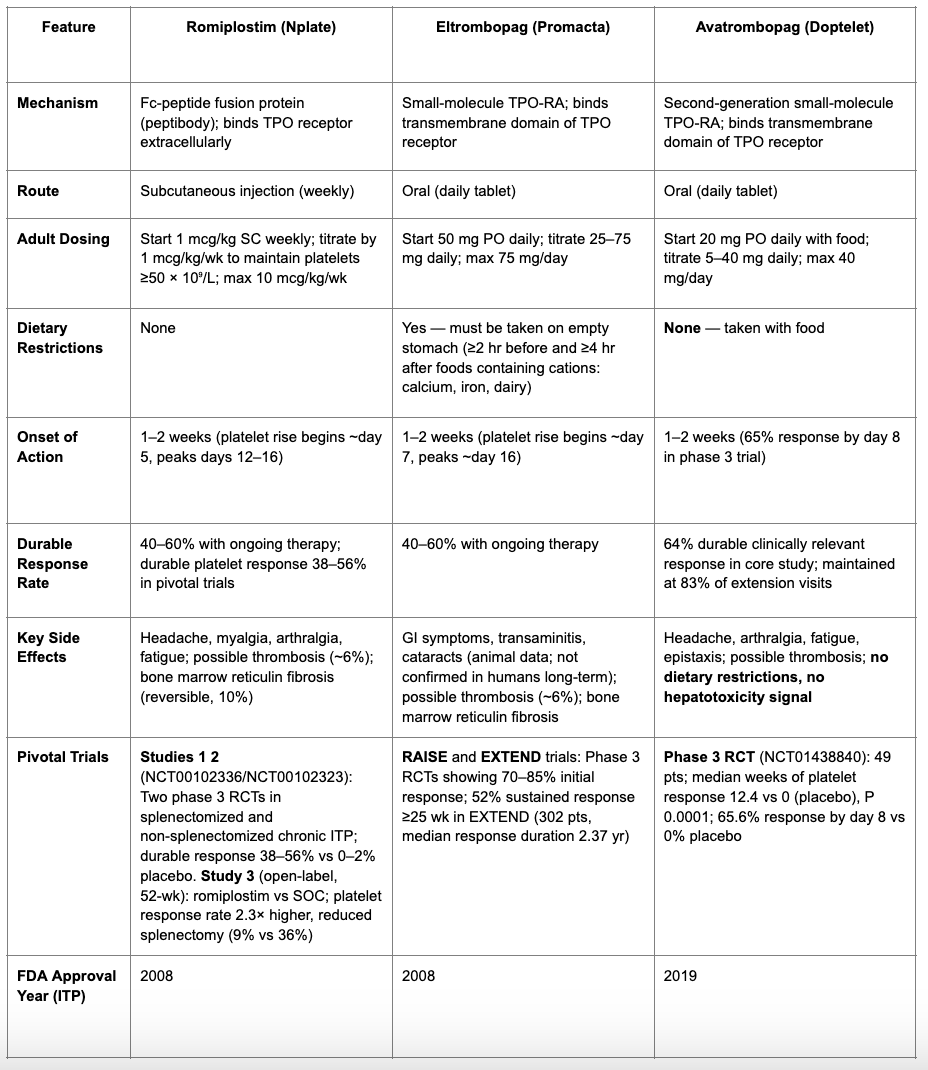
Table 1: Comparisons between TPO-RA options (Chart generated using OpenEvidence, data then reviewed)
What is the role of rituximab in the second-line setting?
Mechanism: An anti-CD20 monoclonal antibody that depletes the B-cell populations responsible for generating the pathogenic autoantibodies driving ITP.
Pros and Cons:
The Upside: It offers a highly convenient, time-limited treatment course—375 mg/m² intravenously once weekly for 4 weeks, and then therapy is complete.
The Downside: It has a slow onset of action (1–8 weeks), making it a poor choice if a patient requires an immediate platelet rescue. It also carries a risk of prolonged immunosuppression and infection.
Expected outcomes: Initial response occurs in roughly 60% of patients, with a durable response maintained at 12 months in about 40% of cases. If a patient eventually relapses, a retrial can be effective, though subsequent remissions are rarely longer than the first.
Critical testing workflow: Rituximab carries a black-box warning for Hepatitis B reactivation.
Clinical Pearl: Ensure Hep B serologies are checked before giving IVIg during the initial hospitalization. IVIg can cause passive antibody transfer, creating a false-positive Hep B surface antibody screen that complicates future rituximab administration.
What does the data show for the newer agents, fostamatinib and rilzabrutinib?
Fostamatinib:
An oral, twice-daily spleen tyrosine kinase (Syk) inhibitor. Syk signaling is crucial for macrophage activation and the subsequent clearance of antibody-coated platelets in the spleen and liver.
FDA-approved based on the pooled FIT-1 and FIT-2 Phase 3 multi-center randomized controlled trials.
Trial Population: Heavily pre-treated chronic ITP patients (platelets <30,000; most had ≥3 prior lines, half failed a TPO-RA, and a third had a prior splenectomy or rituximab).
Efficacy data: Overall response (any platelet count >50,000 in the first 12 weeks) was 43% vs. 14% with placebo. Stable/sustained disease (platelets >50,000 for 4 of the last 6 weeks of trial) was 18% vs. 2% with placebo.
On-target side effects: Average onset is 1–2 weeks. The most common adverse effects to monitor include diarrhea, hypertension, and neutropenia.
Rilzabrutinib:
A highly selective, oral, twice-daily BTK inhibitor evaluated in the 2025 LUNA3 Phase 3 randomized, placebo-controlled trial.
Mechanism: Limits B-cell activation, curtails pathogenic antibody production, and directly blocks macrophage-mediated platelet phagocytosis and associated inflammatory cascades.
Trial Population: A highly refractory cohort with a median ITP duration of 6–8 years and a median of ≥5 prior lines of therapy (including 12% who had failed fostamatinib).
Efficacy data: Durable platelet response (maintaining platelets ≥50,000 for at least 2/3 of weekly checks during the final 12 weeks without rescue) was achieved in 23% of the rilzabrutinib arm compared to 0% in the placebo group.
Clinical benefits: Responders had a median time to response of 15 days, a 52% reduction in the requirement for rescue medications, and significant clinical improvements in both bleeding scores and ITP-related fatigue.
Tolerability: Side effects were predominantly low-grade (Grade 1–2) gastrointestinal upset (diarrhea, nausea) and mild headaches.
To summarize:
When a patient experiences an early relapse after initial frontline therapy, a secondary, short steroid course can be utilized, but long-term management requires a shift toward second-line agents.
In modern practice, second-line management primarily sequences through TPO-RAs or Rituximab, followed by newer targeted pathways like fostamatinib (Syk inhibitor) or rilzabrutinib (BTK inhibitor).
Splenectomy remains highly effective for long-term remission but has transitioned to a later-line rescue option due to irreversible surgical risks and life-long infectious and vascular complications.
The target platelet goal shifts in the second-line setting: we are no longer shooting for normal cell lines, but rather a stable threshold >50,000 to mitigate severe bleeding risk and preserve quality of life.
The crew behind the magic:
Show outline: Ronak Mistry
Production and hosts: Vivek Patel, Dan Hausrath, Ronak Mistry
Editing: Resonate Recordings
Shownotes: Karam Elsolh
Graphics, social media management: Ronak Mistry