Episode 157: Immune Thrombocytopenic Purpura Series, Pt 3- Challenging Scenarios in ITP
This week, we put everything we talked about in our ITP series together and talk about how we manage ITP in complicated patient scenarios. Through a case-based discussion, we discuss how to we would approach each of these complicated scenarios. If you haven’t done so already, be sure to check out episodes 155 and 156!
Case 1: ITP in pregnancy
24 year old otherwise healthy female patient who was diagnosed with ITP. Her baseline platelet count remains consistently in the 80s. She recently became pregnant and is in the first trimester. As part of her pre-natal visits with OB, gets a CBC and platelets are now 34. What do you do?
Differential diagnosis for thrombocytopenia in pregnancy:
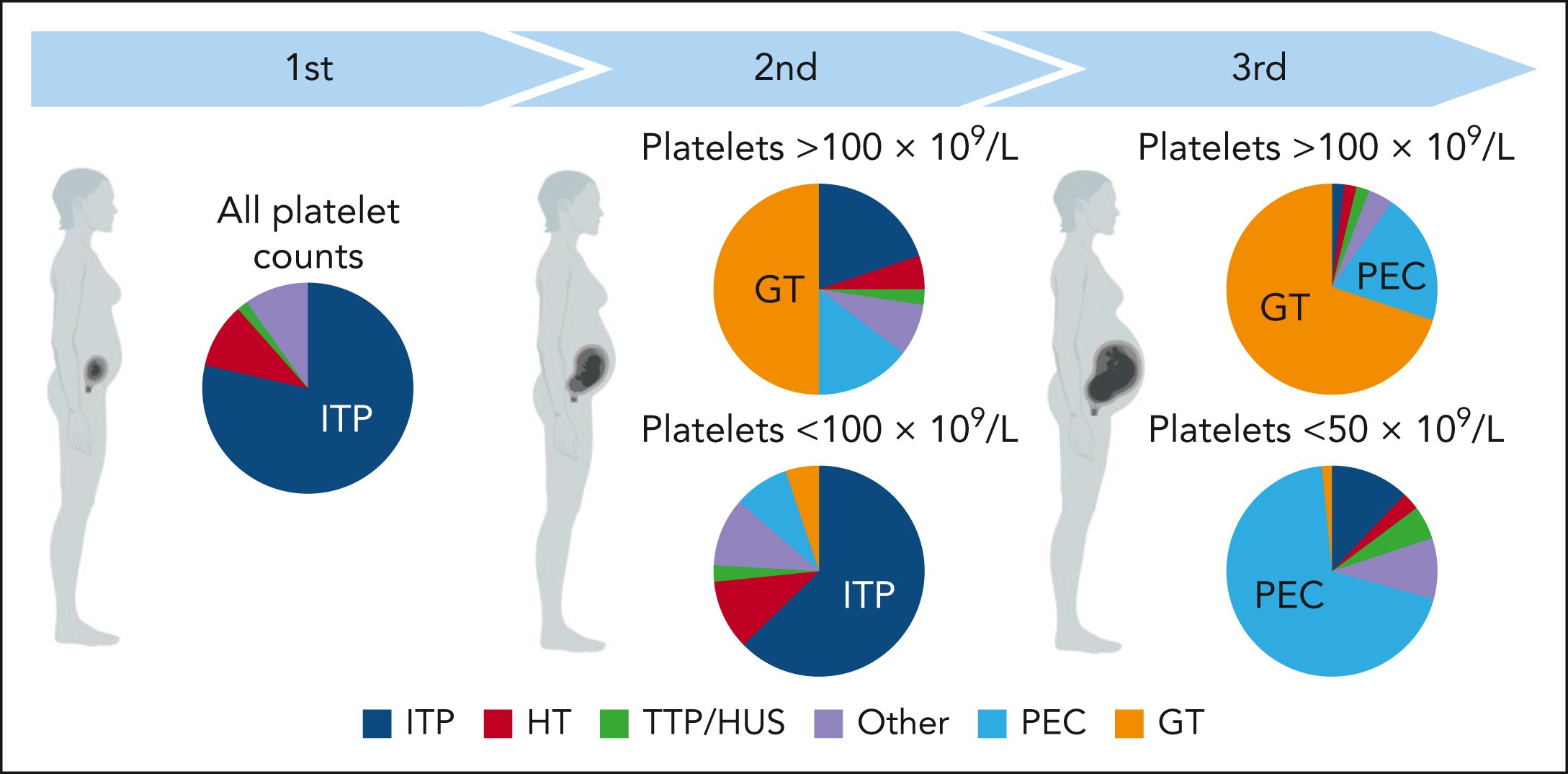
Figure 1: Differential diagnoses for thrombocytopenia in pregnancy. Source: Blood (2024) 143 (9): 747–756. https://doi.org/10.1182/blood.2023020726
Guidelines recommend close observation and not treating in the first 8 months of pregnancy unless platelets <20 or there is bleeding.
In the weeks leading up to the expected due date, this changes. Always check institutional guidelines. In general:
In order to get an epidural, goal platelets >70
If no epidural is desired, most OBs will want platelets >50
If treatment indicated:
Consider IVIg first
Many options: 0.4g/kg x5 days, 1g/kg x2 days, 2g/kg once
This can be considered every few weeks to maintain the platelet counts
If steroids are needed:
Prednisone is preferred over dexamethasone
Dexamethasone crosses the placenta and can cause fetal birth defects
Steroids are usually reserved for the 35 or 36th week to limit maternal side effects
If refractory and platelets remain <20:
Options include rituximab, azathioprine, or cyclosporine. Note: These options take time to work and data are limited in pregnancy.
TPO-RAs do cross the placenta and there are limited data about their use in pregnant patients.
Splenectomy is rarely used, but remains an option.
Case 2: Patient on anticoagulation - stable for discharge?
61 year old male with a past medical history of atrial fibrillation on apixaban who presents with new petechiae and platelet count of 12, other cell lines are normal. Workup is concerning for ITP. Apixaban is held. He is started on dexamethasone 40mg x4 days and IVIG 1g/kg x2 days. On hospital day 5, his platelet count is 43. The primary team inquires about platelet goals.
Typically, therapeutic anticoagulation should be held for platelets <50 therefore the goal platelet threshold should be over 50
Depending on the patient and their bleeding risk, often safe to consider higher threshold (such as minimum platelets 70) to allow for a buffer zone. Important to consider for patients who have a bleeding history.
Case 3: New VTE in a patient with ITP flare
61 year old male with chronic ITP that has been refractory to multiple lines of therapy, but currently responding to eltrombopag. He develops a new PE while on eltrombopag. Platelets at the time were 400. He is started on apixaban and eltrombopag is held. He presents to clinic 1 month later and his platelets are 12.
First prioritize quickly getting platelets up before starting anticoagulation:
Hospitalize
Start IVIg and dexamethasone
Once platelets have improved, start therapeutic anticoagulation
Recall that thrombosis is a risk factor with TPO-RAs. Can still consider use of TPO-RA in this case, as patient was responding/refractory to other therapies. Consider a lower dose.
If patient is uncomfortable restarting, consider other options (for example: fostamatinib, rilzabrutinib)
Case 4: Acute life-threatening bleeding with ITP flare
81 year old male with a new spontaneous subdural hematoma found to have a platelet count of 12. Workup consistent with ITP.
A multipronged approach is what is recommended here using combination therapy:
High dose steroids with either dex 40 IV; many would even use IV methylprednisolone 1g
Add IVIg 1g/kg
Highly consider platelet transfusions
Also consider adding TPO-RA
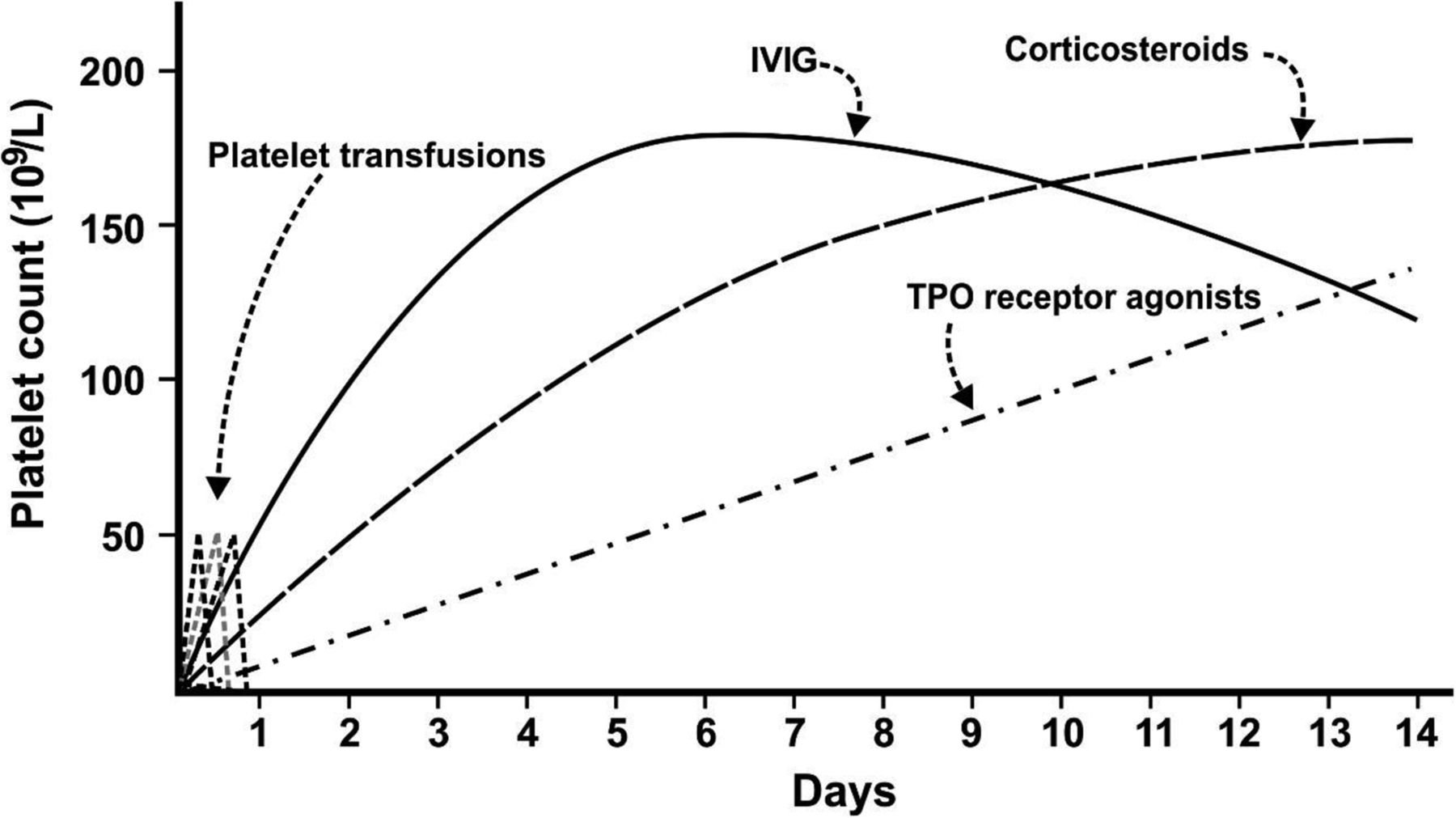
Figure 2: Onset of action of agents in management of ITP in acute bleeding. Source: Hematology Am Soc Hematol Educ Program (2015) 2015 (1): 237–242. https://doi.org/10.1182/asheducation-2015.1.237
Case 5: Refractory ITP despite multiple therapies
64 year old male with a prior history of head and neck cancer s/p chemoradiation with presents with petechiae and gum bleeding, platelets <10. Despite multiple therapies (steroids, IVIg) he is not responding.
Remember that ITP is a diagnosis of exclusion
In a patient with a history of malignancy, consider ?MDS vs. marrow infiltration
In a patient with recent chemoradiation, consider toxic effects of therapy
In situations like this, want to consider bone marrow biopsy +/- additional workup/imaging
What is “refractory ITP”? Since we don’t use splenectomy as often, which was part of the old definition, the current definition is a lack of response to 2 or more rescue and/or disease modifying treatments with or without bleeding manifestations
See excellent review article about “refractory” case
Some important facts:
50% of refractory ITP is really primary ITP
10% of ITP is secondary
15% is another inherited form of thrombocytopenia
10% is bone marrow failure
10% is MDS
5% is drug induced
Case 6: Refractory ITP despite multiple therapies
Let’s say that the patient above underwent a bone marrow biopsy and testing was normal. He has now received several courses of steroids, IVIg, eltrombopag x3 weeks and still does not have a platelet response. What are next steps?
Consider switching to another TPO-RA
Review medications to ensure no possibility of drug-induced ITP
Evaluate for ectopic spleen/splenule
Refractory cases of ITP can evolve from a B-cell process to a T-cell process. Therefore use of medications such as mycophenolate or cyclosporine may need to be considered.
May need to consider splenectomy
Need vaccines to pneumococcus, meningitis and H.influenza; ideally at least 2 weeks prior to elective surgery; if urgent, then prior to hospital discharge or within 2 weeks, whichever comes first.
Thromboprophylaxis for 2 weeks after surgery
Link to vaccine schedule
Case 7: TPO-RA intolerance
55M with ITP on TPO-RA with platelet response now with myalgias impairing quality of life. What do we do next?
If myalgias/arthralgias are minor, consider use of as needed acetaminophen (avoid NSAIDs, especially if thrombocytopenic)
If severe, consider switching to a different TPO-RA
If this still doesn’t work, then switch to a different class of drugs
The crew behind the magic:
Show outline: Ronak Mistry
Production and hosts: Vivek Patel, Dan Hausrath, Ronak Mistry
Editing: Resonate Recordings
Shownotes: Ronak Mistry
Graphics, social media management: Ronak Mistry