Episode 142: Myeloma Series, Pt.3 - Management of Smoldering Multiple Myeloma (2025)
The way that we think about smoldering multiple myeloma (SMM) has continued to see evolution in the plasma cell dyscrasia space. If this diagnosis portends a higher risk of developing multiple myeloma, how should we manage patients to prevent possible end-organ damage? Is it a one-size-fits-all approach or are there some patients who are higher risk for progression than others? We cover this and so much more in this new episode!

This episode is brought you by Primum: Connect with hematology and oncology specialists for real-time curbside consults at no cost to you!
A quick reminder on MGUS.
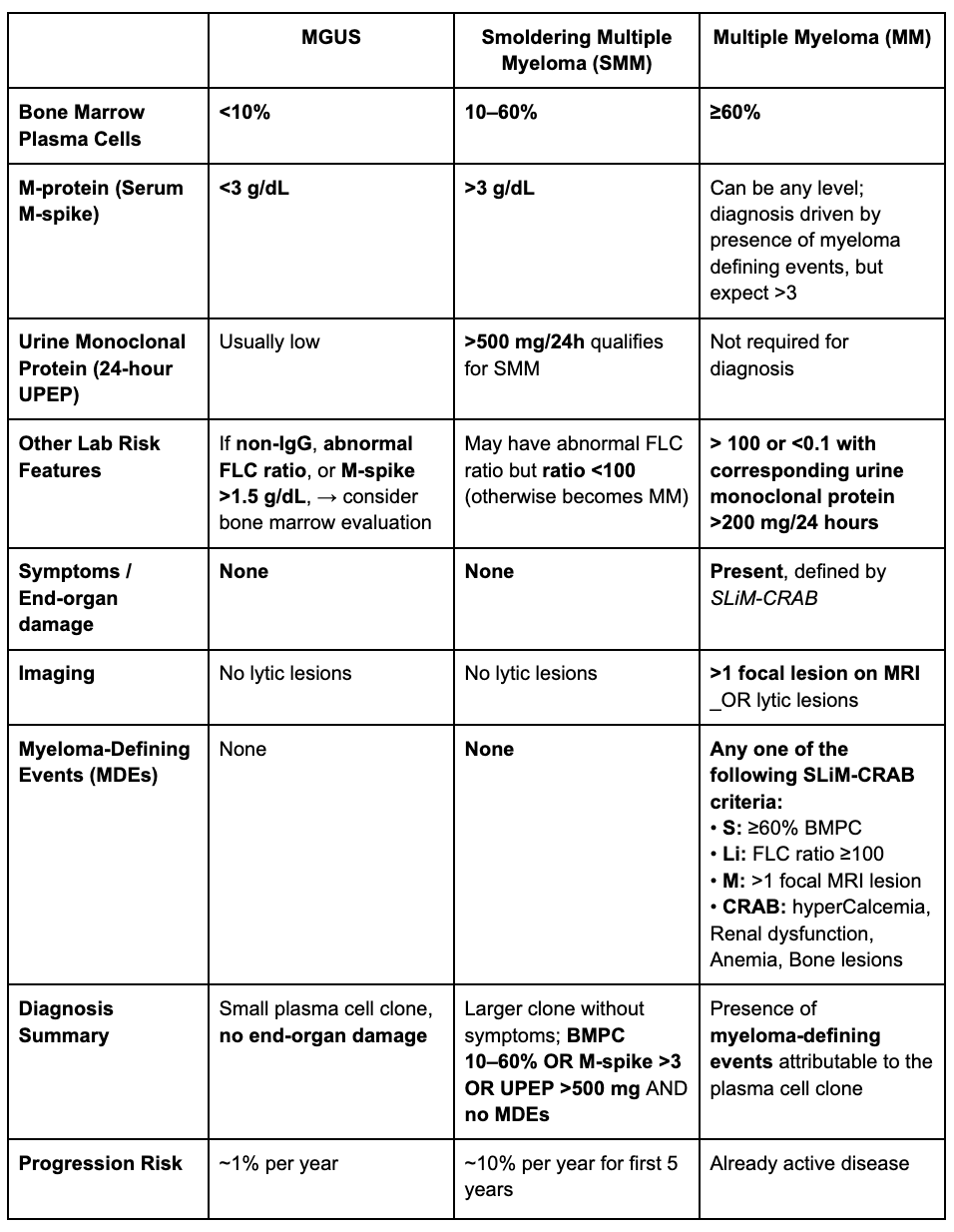
MGUS is defined by:
Monoclonal protein quantity (M-spike) <3 g/dL
<10% plasma cells in bone marrow
No “myeloma defining events” (more below)
If one or more of the criteria above are met, then you do a bone marrow biopsy and either whole body PET/CT or MRI to evaluate for lytic lesions.
How do we define Smoldering Myeloma (SM)?
Must have one of the following
M protein >3 g/dL (serum) OR
≥ 500mg monoclonal protein/24h (urine) OR
Clonal plasma cells in BM ≥ 10%-60%
AND no myeloma defining events
What are “myeloma defining events”?
SLiMCRAB Criteria
S: ≥60% clonal plasma cells in BM
Li: Light chain ratio>100 or <0.1
Should also have corresponding urine monoclonal protein >200 mg/24 hours (Visram et al. Leukemia 2022)
Study showed that free light chain difference > 100 and urine < 200 was same risk as free light chain < 100 → another reason why a 24 hour UPEP is so important
M: MRI showing >1 focal lesion (>5mm in size)
C: HyperCalcemia: >11mg/dl
R: Renal insufficiency: CrCl<40 or Serum Cr>2
A: Anemia: <10 g/dl or 2g/dl below normal for that patient
B: Bone lesions: ≥1 bone lesions on CT, PET CT or bone radiographs.
How common is MGUS?
MGUS is incredibly common in ~5% of the adult population and the risk of progression is a ballpark of 1% per year.
A study from the Mayo group looked at 1384 patients, equating to 11,009 person-years of follow-up, and found that 1% of those patients progressed.
In 2007, the same group released a study looking at the progression of smoldering myeloma over a 26 year period, equating to 2131 person years of follow up. They reported the risk of progression in the first 5 years was 10%, followed by 3% per year for the next 5 years, followed by 1% per year for the remaining 10 years. This cumulative risk of progression over 15 years is 73%.
Would you consider MGUS “a cancer?”
MGUS is very common and does NOT equal cancer.
MGUS is similar to CLL RAI stage 0. Asymptomatic and live normal lives. We could have named this multiple myeloma stage 0, meaning 5% of the population would have “stage 0 multiple myeloma”.
Who defined smoldering myeloma?
For a historical context, Dr. Bob Kyle defined smoldering myeloma in a paper in NEJM 1980.
Prior to this time, myeloma was serologically defined by M protein > 3 and BMPC > 10% regardless of classic CRAB criteria.
His group followed 6 patients meeting this criteria and none progressed, resulting in the new terminology of smoldering myeloma.
What is the prevalence of smoldering myeloma?
An Icelandic study showed an estimated prevalence of ~0.5% of the adult population over the age of 40 has SMM.
They have an initiative called iStopMM study (Iceland Screens Treats or Prevents Multiple Myeloma) which screened over 75,000 healthy patients with SPEP and serum free light chains.
How to think about MGUS→SM→MM progression (Using the colon polyp analogy)
Not all polyps become colon cancer, but some carry higher risk features, necessitating more frequent monitoring. MGUS and SM follow the same logic.
Initial clone formation: The first genetic hit, depending on the number and type of abnormalities creates the plasma cell clone which presents clinically as MGUS or SM.
Risk assessment gap: Unlike AML, we do not currently have a molecular risk profile to assess risk of progression.
MGUS progression: Patients with MGUS have a steady 1% per year risk of progression meaning there is a low chance of another “hit” to the genome leading to malignant transformation.
SM progression: This same idea can be true for smoldering myeloma but we know that some of these patients tend to progress earlier meaning they have a genome that has a higher chance for those additional hits- particularly in the first 5 years
What Defines Higher-Risk Smoldering Myeloma?
High-risk SMM refers to biologic or clinical features associated with a ≥50% risk of progression to symptomatic myeloma within 2 years. The most widely used predictors include:
Clinical Risk Features — “20-2-20 Rule” (Mayo 2018 Model)
High-risk status is defined by ≥2 of the following:
M-protein ≥2 g/dL
Involved/uninvolved FLC ratio ≥20
Bone marrow plasma cells ≥20%
Patients meeting 2–3 criteria have >50% 2-year progression risk
High Risk Cytogenetic Abnormalities:
Identified by FISH and strongly associated with earlier progression:
t(14;16)
t(14;20)
t(4;14)
del(17p)
1q abnormalities
Note: 1q21 gain is sometimes included but is biologically distinct from 1q amplification, and amplification (>3 copies) is the feature consistently associated with high-risk disease.
Landmark trials in Smoldering Myeloma
When we talk about shifting from “watch and wait” to early therapeutic intervention in smoldering myeloma, a handful of landmark trials define the entire landscape. These studies shaped how we think about high-risk biology, timing of treatment, and what outcomes actually matter for patients.
The QuiRedex Trial (2013)
QuiRedex study was the first randomized trial to show that treating high-risk smoldering myeloma early (lenalidomide + dexamethasone) delayed progression and even suggested a survival benefit compared to observation.
This trial sparked a question in the field: If we can identify patients likely to progress, should we act before irreversible organ damage occurs?
ECOG E3AO6 (2020)
A randomized controlled trial evaluating lenalidomide vs. observation in patients with intermediate- or high-risk SMM as defined by the 2008 criteria..
Lenalidomide maintained superior progression-free survival at 1, 2, and 3 years—98%, 93%, and 91% versus 89%, 76%, and 66% with observation with a hazard ratio of 0.28.
Take away: Treat patients with the highest risk SM. FDA said no approval since there was no OS benefit.
Limitations: No demonstrated overall survival benefit, leading to lack of FDA approval; the study also did not capture end-organ progression such as fractures or renal decline, which are clinically meaningful outcomes.
AQUILA Trial (2025):
A phase 3, open-label, multicenter study evaluating daratumumab vs active surveillance in patients with high-risk SMM (ECOG 0–1), defined by features such as:
M-protein >3 g/dl
IgA subtype
FLC ratio >8
10–60% bone marrow plasma cells
All patients were required to undergo PET-CT and whole-body MRI for accurate staging
Primary endpoint: Progression-free survival (PFS)
Primary endpoint: Progression-free survival (PFS)
5-year PFS: 63.2% with daratumumab vs. 40.8% with active monitoring
Hazard ratio: 0.49, demonstrating a clear delay in progression.
Clinical takeaway: NCCN now lists daratumumab as an option for high-risk SMM, reflecting growing acceptance of early intervention.
Concerns: Are we overtreating patients? Are patients progressing and not receiving treatment for MM?
This episode is brought you by Primum: Connect with hematology and oncology specialists for real-time curbside consults at no cost to you!
References:
Kyle RA, Therneau TM, Rajkumar SV, Offord JR, Larson DR, Plevak MF, Melton LJ 3rd. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med. 2002 Feb 21;346(8):564-9. doi: 10.1056/NEJMoa01133202. PMID: 11856795.
Kyle RA, Remstein ED, Therneau TM, Dispenzieri A, Kurtin PJ, Hodnefield JM, Larson DR, Plevak MF, Jelinek DF, Fonseca R, Melton LJ 3rd, Rajkumar SV. Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med. 2007 Jun 21;356(25):2582-90. doi: 10.1056/NEJMoa070389. PMID: 17582068.
Lonial S, Jacobus S, Fonseca R, Weiss M, Kumar S, Orlowski RZ, Kaufman JL, Yacoub AM, Buadi FK, O'Brien T, Matous JV, Anderson DM, Emmons RV, Mahindra A, Wagner LI, Dhodapkar MV, Rajkumar SV. Randomized Trial of Lenalidomide Versus Observation in Smoldering Multiple Myeloma. J Clin Oncol. 2020 Apr 10;38(11):1126-1137. doi: 10.1200/JCO.19.01740. Epub 2019 Oct 25. PMID: 31652094; PMCID: PMC7145586.
Mateos MV, Hernández MT, Giraldo P, de la Rubia J, de Arriba F, López Corral L, Rosiñol L, Paiva B, Palomera L, Bargay J, Oriol A, Prosper F, López J, Olavarría E, Quintana N, García JL, Bladé J, Lahuerta JJ, San Miguel JF. Lenalidomide plus dexamethasone for high-risk smoldering multiple myeloma. N Engl J Med. 2013 Aug 1;369(5):438-47. doi: 10.1056/NEJMoa1300439. PMID: 23902483.
Dimopoulos MA, Voorhees PM, Schjesvold F, Cohen YC, Hungria V, Sandhu I, Lindsay J, Baker RI, Suzuki K, Kosugi H, Levin MD, Beksac M, Stockerl-Goldstein K, Oriol A, Mikala G, Garate G, Theunissen K, Spicka I, Mylin AK, Bringhen S, Uttervall K, Pula B, Medvedova E, Cowan AJ, Moreau P, Mateos MV, Goldschmidt H, Ahmadi T, Sha L, Cortoos A, Katz EG, Rousseau E, Li L, Dennis RM, Carson R, Rajkumar SV; AQUILA Investigators. Daratumumab or Active Monitoring for High-Risk Smoldering Multiple Myeloma. N Engl J Med. 2025 May 8;392(18):1777-1788. doi: 10.1056/NEJMoa2409029. Epub 2024 Dec 9. PMID: 39652675.
The crew behind the magic:
Show outline: Vivek Patel, Sean Taasan
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath, Sean Taasan
Editing: Resonate Recordings
Shownotes: Megan Connor
Graphics, social media management: Ronak Mistry